|
Overview
 Flat feet and fallen arches are common conditions that are in most cases asymptomatic. However, in patients who do have symptoms, treatments are available that can help reduce pain and promote efficient movement. Orthotic devices are well recognised as an excellent treatment and podiatrists can offer these different treatment modalities as individualised treatments for patients. Causes There are a number of different causes that can lead to flat feet or fallen arches. These include, birth defects, while technically not a defect as such, flat feet can be a normal finding in patients from birth. However, a condition called tarsal coalition may occur where some of the bones in the foot are fused together resulting in a flatfoot. Inflammation or damage of the posterior tibial tendon. This tendon forms the end of a muscle that connects the lower leg to the foot, winding around the ankle and attaching to the inner aspect where the arch is normally present. The main role of the posterior tibial tendon is to invert the foot and maintain the arch height throughout the gait cycle. Torn muscles of the leg and foot can cause flat feet. Problems with the nerve supply to the muscles can result in reduction in tone and fallen arches. Fracture dislocation of the bones in the foot. Severe arthritis. While these are the common causes that can result in fallen arches and flat feet, it is important to recognise that there are certain risk factors that can also lead to this condition. These include advancing age, diabetes mellitus, high blood pressure, obesity and pregnancy. Symptoms Feet tire easily and become painful and achy, especially around the arch, ankle and heel. Swelling on the inside bottom of your feet. Back and leg pain. Difficulty standing on toes. Diagnosis You can test yourself to see if you have flat feet or fallen arches by using a simple home experiment. First, dip your feet in water. Then step on a hard flat surface, like a dry floor or a piece of paper on the floor, where your footprints will show. Step away and examine your foot prints. If you see complete/full imprints of your feet on the floor, you may have fallen arches. However, it?s important to seek a second option from a podiatrist if you suspect you have fallen arches so they can properly diagnose and treat you. pes planus treatment Non Surgical Treatment If fallen arches are not causing any pain or discomfort, then they will not need any treatment. If they were causing a persistent pain in the feet, or in the hips, legs or knees, then it would be best to consult your family doctor. Walking is the natural activity of feet and if it is not too painful, sufferers should walk as much as possible to strengthen their arches. When it is possible, go barefoot, or wear soft flexible shoes. In cases of severe fallen arches, your doctor may recommend special shoe inserts. Surgical Treatment  A combination of surgical procedures can be used to reconstruct the flatfoot. Generally, these procedures can be separated into those that correct deformities of the bones and those that repair ligaments and tendons. Your orthopaedic surgeon will choose the proper combination of procedures for your foot. Surgery of the foot can be performed under regional anesthesia, which is numbing the foot and ankle with a nerve or spinal block, or general anesthesia, which may require a breathing tube. A nerve block is often placed behind the knee to reduce pain after surgery. Prevention Wear Supportive Footwear. Spend the money it takes to get proper fitting and quality footwear with good arch supports. Most sufferers of fallen arches and plantar fasciitis are born with high arches that sag as they get older. Good footwear can prevent this from becoming a problem. Flat feet, however, can become just as problematic. So, really we should all be wearing good footwear to avoid this potentially painful condition. Take It Easy. If your heel starts to hurt, take a rest. If the pain doesn?t go away after several days of resting, it may be time to see a podiatrist. Orthotics. Special insoles to support the arch of the foot can provide some much needed help. You can buy these at your local drugstore (not recommended), or you can have them specially made and custom fit for your feet. It can take awhile to get just the right one for your foot, but sometimes it can be just what you needed. Weight Control. Yes, maintaining a sensible diet with your ideal weight can be beneficial in many ways. It makes sense to think that the more weight your arches are supporting, the more easily they will fall and become painful. After Care Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon. Overview
Leg length discrepancy, or as it has been alternatively termed, the short leg syndrome, is by far the most important postural asymmetry. Limb length discrepancy is simply defined as a condition where one leg is shorter than the other. If a substantial difference exists, disruptive effects on gait and posture can occur. Leg length discrepancy can be divided into two etiological groups. Structural. True shortening of the skeleton from congenital, traumatic or diseased origins. Functional. Development from altered mechanics of the lower body, such as foot hyperpronation or supination, pelvic obliquity, muscle/joint imbalances, poor trunk stabilization and deep fascial strain patterns.  Causes The causes of LLD are many, including a previous injury, bone infection, bone diseases (dysplasias), inflammation (arthritis) and neurologic conditions. Previously broken bones may cause LLD by healing in a shortened position, especially if the bone was broken in many pieces (comminuted) or if skin and muscle tissue around the bone were severely injured and exposed (open fracture). Broken bones in children sometimes grow faster for several years after healing, causing the injured bone to become longer. Also, a break in a child?s bone through a growth center (located near the ends of the bone) may cause slower growth, resulting in a shorter extremity. Bone infections that occur in children while they are growing may cause a significant LLD, especially during infancy. Bone diseases may cause LLD, as well; examples are neurofibromatosis, multiple hereditary exostoses and Ollier disease. Inflammation of joints during growth may cause unequal extremity length. One example is juvenile rheumatoid arthritis. Osteoarthritis, the joint degeneration that occurs in adults, very rarely causes a significant LLD. Symptoms Back pain along with pain in the foot, knee, leg and hip on one side of the body are the main complaints. There may also be limping or head bop down on the short side or uneven arm swinging. The knee bend, hip or shoulder may be down on one side, and there may be uneven wear to the soles of shoes (usually more on the longer side). Diagnosis There are several orthopedic tests that are used, but they are rudimentary and have some degree of error. Even using a tape measure with specific anatomic landmarks has its errors. Most leg length differences can be seen with a well trained eye, but I always recommend what is called a scanagram, or a x-ray bone length study (see picture above). This test will give a precise measurement in millimeters of the length difference. Non Surgical Treatment People with uneven leg lengths may be more prone to pain in their back, hips, and knees; uneven gait; and lower leg and foot problems. Due to its risks, surgery is typically not recommended unless the difference is greater than one inch. In cases where the difference is less than one inch, providing the same support for both feet is the most effective. This can be achieved by getting custom-fitted orthotics for both feet. Orthotics are inserts that you wear in the shoes. Your chiropractor will request to measure your feet and possibly your legs. You can step on a device that will take the measurements or you might have a plaster cast of your feet taken. Orthotics are typically made from plastic and leather, and function biomechanically with your foot. If a leg length discrepancy is not properly corrected with orthotics, your chiropractor may recommend a heel lift, also known as a shoe lift. You simply place it in the back of your shoe along with the orthotic. Typically, you will only wear the heel lift in one shoe to assist the shorter leg.  shoe lifts for height Surgical Treatment Many people undergo surgery for various reasons - arthritis, knee replacement, hip replacement, even back surgery. However, the underlying cause of leg length inequality still remains. So after expensive and painful surgery, follow by time-consuming and painful rehab, the true culprit still remains. Resuming normal activities only continues to place undue stress on the already overloaded side. Sadly so, years down the road more surgeries are recommended for other joints that now endure the excessive forces. Overview
 Morton neuromas are focal areas of symptomatic perineural fibrosis around a plantar digital nerve of the foot. The abnormality is non-neoplastic and does not represent a true neuroma. It may more correctly be known as Morton?s metatarsalgia. The condition is thought to be due to chronic entrapment of the nerve by the intermetatarsal ligament. It most often occurs in middle-aged individuals and is many times more common in women than men. Approximately 30% of asymptomatic middle-aged persons have the radiological pathologic findings of a Morton?s neuroma. Morton neuromas are focal areas of symptomatic perineural fibrosis around a plantar digital nerve of the foot. The abnormality is non-neoplastic and does not represent a true neuroma. It may more correctly be known as Morton?s metatarsalgia. The condition is thought to be due to chronic entrapment of the nerve by the intermetatarsal ligament. It most often occurs in middle-aged individuals and is many times more common in women than men. Approximately 30% of asymptomatic middle-aged persons have the radiological pathologic findings of a Morton?s neuroma.Causes Poorly fitted footwear can be a cause. Shoes that have a tight and narrow toe box can cause the never to become entrapped causing the pain. High heeled shoes abnormally place the metatarsals under extreme pressure which can cause Morton?s Neuroma. In cases of abnormal pronation, there can be significant motion between the 3rd and 4th metatarsals which can cause an irritation to the nerve that runs between them. This inflammation causes the pain. Symptoms The symptoms of Morton?s Neuroma tend to come and go over time. They are typically exacerbated by physical activity or by wearing certain shoes. Morton?s Neuroma symptoms include sharp pain in the ball of the foot, pain radiating to the tips of the toes, burning pain in the second, third, or fourth toes, numbness in the toes, sensation of a lump between the toes. Diagnosis Your doctor will suspect that you have a Morton's neuroma based on the nature and location of your foot pain. He or she may ask questions about your shoes - what type of shoes you usually wear and whether these shoes have narrow toes or high heels. To rule out other causes of foot pain, your doctor may ask questions about your medical history, especially any history of arthritis, nerve and muscle problems or previous injury to your foot or leg. Non Surgical Treatment Most non-operative treatment is usually successful, although it can take a while to figure out what combination of non-operative treatment works best for each individual patient. Non-operative treatment may include the use of comfort shoe wear. The use of a metatarsal pad to decrease the load through the involved area of the plantar forefoot. A period of activity modification to decrease or eliminate activities, which may be exacerbating the patient?s symptoms. For example, avoiding long periods of standing or other activities that result in significant repetitive loading to the forefoot can be very helpful. Wearing high heels should be avoided. Local can help decrease inflammation associated with the nerve. However, this does not necessarily address the underlying loading forces that maybe causing the injury to the nerve in the first place. It has been proposed that an alcohol injection in and around the nerve will cause a controlled death to the nerve and subsequently eliminate symptoms. In theory, this may be helpful. In practice, adequate prospective studies have not demonstrated the benefit of this procedure above and beyond the other standard, non-operative treatments available. In addition there is the concern that the alcohol will cause excessive scarring and damage to other important structures in the area.  Surgical Treatment Should the problem have progressed beyond the point where these measures are sufficient, the podiatric professional may recommend surgery. This procedure involves excision of the involved nerve mass. This will relieve the pain. Many patients report permanent numbness in the spot formerly affected by the neuroma, but prefer it to the pain. Most surgeries are successful; unfortunately, there are cases where the patient suffers another neuroma, sometimes in or near the same spot as before. A podiatric professional can explain the statistics of recurrence in various cases. If you suspect a neuroma, don?t wait for it to get better on its own. The earlier the diagnosis, the higher the likelihood that it can be treated with conservative measures. Don?t think that foot pain of any kind is inevitable, either, even if it runs in your family.  Overview OverviewHammer Toe most commonly affects the second toe on the foot. It causes the middle joint to bend. Hammertoe is most frequently caused by structural problems in the toe or from wearing poor fitting shoes. It is important to diagnose and treat hammertoe early because the condition tends to become worse over time. If left untreated, hammertoe can require surgery. Causes Risk factors for hammertoe include heredity, a second toe that is longer than the first (Morton foot), high arches or flat feet, injury in which the toe was jammed, rheumatoid arthritis, and, in diabetics, abnormal foot mechanics resulting from muscle and nerve damage. Hammertoe may be precipitated by advancing age, weakness of small muscles in the foot (foot intrinsic muscles), and the wearing of shoes that crowd the toes (too tight, too short, or with heels that are too high). The condition is more common in females than in males.  Symptoms People who have painful hammertoes visit their podiatrist because their affected toe is either rubbing on the end their shoe (signaling a contracted flexor tendon), rubbing on the top of their shoe (signaling a contracted extensor tendon), or rubbing on another toe and causing a painful buildup of thick skin, known as a corn. Diagnosis Hammertoes are progressive, they don?t go away by themselves and usually they will get worse over time. However, not all cases are alike, some hammertoes progress more rapidly than others. Once your foot and ankle surgeon has evaluated your hammertoes, a treatment plan can be developed that is suited to your needs. Non Surgical Treatment Your doctor will decide what type of hammertoe you have and rule out other medical conditions. Treatment may range from more appropriate footgear to periodic trimming and padding of the corn. Cortisone injections may be indicated if a bursitis is present. Antibiotics may be utilized in the presence of infection. Removable accommodative pads may be made for you. Surgical Treatment Toes can be surgically realigned and made straight again. They can even be made shorter. The good news is that toes can be corrected. Hammer toe surgery is often synonymous with ?toe shortening?, ?toe job? and/or ?toe augmentation?. Depending on the severity and length of the toe, there are several methods to surgically correct a hammer toe. In general, the surgery involves removing a portion of the bone at the contracted joint, to realign the toe.
Overview
 A bunion is generally considered as an enlargement of the joint (a lump of bone) at the base and side of the big toe (specifically, the first metatarsophalangeal joint). Bunions form when the toe moves out of place. As the big toe bends towards the others this lump becomes larger and the bunion can become painful, arthritis and stiffness can eventually develop. Hallux valgus or hallux abducto valgus (HAV) is the name used for the deviated position of the big toe and a bunion refers to the enlargement of the joint, most of the time the two go together and can just be referred to as 'bunions'. The word bunion is from the Latin "bunion," meaning enlargement. A bunion is generally considered as an enlargement of the joint (a lump of bone) at the base and side of the big toe (specifically, the first metatarsophalangeal joint). Bunions form when the toe moves out of place. As the big toe bends towards the others this lump becomes larger and the bunion can become painful, arthritis and stiffness can eventually develop. Hallux valgus or hallux abducto valgus (HAV) is the name used for the deviated position of the big toe and a bunion refers to the enlargement of the joint, most of the time the two go together and can just be referred to as 'bunions'. The word bunion is from the Latin "bunion," meaning enlargement.Causes A true bunion or hallux valgus results from a drifting inwards of the big toe metatarsal from its normal position closer to the second metatarsal. The bunion is the head of this first metatarsal which produces the prominence on the inner side of the now wider foot. Tendons run circumferentially around the metatarsal and toe. They both move and stabilise the toe under normal circumstances. In a bunion or hallux valgus, with the shift/displacement of the first metatarsal these tendons no longer lie in the correct axis and in fact act as a deforming force, contributing to the bunion condition. Symptoms Just because you have a bunion does not mean you have to have pain. There are some people with very severe bunions and no pain and people with mild bunions and a lot of pain. Symptoms for a bunion may include pain on the inside of your foot at the big toe joint. Swelling on the inside of your foot at the big toe joint. Redness on the inside of your foot at the big toe joint. Numbness or burning in the big toe (hallux). Decreased motion at the big toe joint. Painful bursa (fluid-filled sac) on the inside of your foot at the big toe joint. Pain while wearing shoes, especially shoes too narrow or with high heels. Joint pain during activities. Other conditions which may appear with bunions include corns in between the big toe and second toe. Callous formation on the side or bottom of the big toe or big toe joint. Callous under the second toe joint. Pain in the second toe joint. Diagnosis Physical examination typically reveals a prominence on the inside (medial) aspect of the forefoot. This represents the bony prominence associated with the great toe joint ( the medial aspect of the first metatarsal head). The great toe is deviated to the outside (laterally) and often rotated slightly. This produces uncovering of the joint at the base of the big toe (first metatarsophalangeal joint subluxation). In mild and moderate bunions, this joint may be repositioned back to a neutral position (reduced) on physical examination. With increased deformity or arthritic changes in the first MTP joint, this joint cannot be fully reduced. Patients may also have a callus at the base of their second toe under their second metatarsal head in the sole of the forefoot. Bunions are often associated with a long second toe. Non Surgical Treatment Some bunions can be treated without surgery. If you have a bunion, wear shoes that are roomy enough so that they won?t put pressure on it. You can choose to have your shoes stretched out professionally or try cushioning the painful area with protective pads. Orthotics have been shown to help prevent progression of bunions. Oral nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, may be recommended to reduce pain and inflammation. Applying an ice pack several times a day can also help reduce inflammation and pain. If your bunion progresses to a point where you have difficulty walking or experience pain even with accommodative shoes, surgery may be necessary. Surgical Treatment The main goal of surgery is to realign the big toe joint in order to relieve symptoms, correct deformity and restore function. Surgery to remove a bunion is known as a bunionectomy. There are many variations of this operation and the type of surgery performed will vary depending on factors such as the degree of deformity, the strength of the bones, the person's age and the surgeon?s preferred approach. Most surgery involves the removal of the bony outgrowth (exostosis) and the realignment of the bones of the joint. Soft tissue structures such as the ligaments and tendons may be repositioned and the bursa may be removed. The insertion of screws and pins may be required to stabilise the bones in their new, realigned position. Prevention Here are some tips to help you prevent bunions. Wear shoes that fit well. Use custom orthotic devices. Avoid shoes with small toe boxes and high heels. Exercise daily to keep the muscles of your feet and legs strong and healthy. Follow your doctor?s treatment and recovery instructions thoroughly. Unfortunately, if you suffer from bunions due to genetics, there may be nothing you can do to prevent them from occurring. Talk with your doctor about additional prevention steps you can take, especially if you are prone to them. Overview
During initial contact or heel strike, the ankle rolls inward, causing excessive pronation or flattening of the foot. This action forces the big toe (instead of the ball of foot and all toes) to do all the work to push off the ground. When the ankle overpronates, this causes the tibia (shin bone) to rotate and the femur (thigh bone) to adduct (move toward the mid-line of the body), causing internal rotation or knee valgus (knock-kneed).  Causes Over-pronation has different causes. Obesity, pregnancy, age or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. Over-pronation is also very common with athletes, especially runners and most of them nowadays use orthotics inside their shoes. Over-pronation affects millions of people and contributes to a range of common complaints including sore, aching feet, ball of foot pain, heel Pain, achilles tendonitis, bunions, shin pain, tired, aching legs, knee pain and lower back pain. The most effective treatment solution for over-pronation is wearing an orthotic shoe insert. Orthotics correct over-pronation, thereby providing natural, lasting pain relief from many common biomechanical complaints. Symptoms It is important to note that pronation is not wrong or bad for you. In fact, our feet need to pronate and supinate to achieve proper gait. Pronation (rolling inwards) absorbs shock and supination (rolling outwards) propels our feet forward. It is our body?s natural shock-absorbing mechanism. The problem is over-pronation i.e. the pronation movement goes too deep and lasts for too long, which hinders the foot from recovering and supinating. With every step, excess pronation impedes your natural walking pattern, causing an imbalance in the body and consequent excessive wear and tear in joints, muscles and ligaments. Some common complaints associated with over-pronation include Heel Pain (Plantar Fasciitis) ,Ball of foot pain, Achilles Tendonitis, Shin splints, Knee Pain, Lower Back Pain. Diagnosis If you have flat feet or low arches, chances are you overpronate. Although not always the case, the lower your arches the greater the overpronate. Stand on a hard surface (in front of a mirror if you need to) and look at your feet, flat feet or low arches are easy to spot. If your feet look flatter than a pancake, have a look at your ankles and see if they seem collapsed or straight. If they are, you're overpronating.  Non Surgical Treatment Personal orthotics can be prescribed via your healthcare professional. If finances or insurance are issues, similar and often better options can be purchased online for overpronation. The right walking shoes are also essential. Most shoes cater to neutral foot gaits, unless they specifically state otherwise. That won?t help you if your foot rolls inward. In order to correct the issue, you need shoes with stability or motion control abilities, low heels, deep heel cups, and good arch support. Surgical Treatment The MBA implant is small titanium device that is inserted surgically into a small opening between the bones in the hind-mid foot: the talus (ankle bone) and the calcaneus (heel bone). The implant was developed to help restore the arch by acting as a mechanical block that prevents the foot from rolling-in (pronation). In the medical literature, the success rate for relief of pain is about 65-70%. Unfortunately, about 40% of people require surgical removal of the implant due to pain. Overview
Sever disease, first described in 1912, is a painful inflammation of the calcaneal apophysis. It is classified with the child and adolescent nonarticular osteochondroses. (The other disease in this group is Iselin disease, which is inflammation of the base of the fifth metatarsal.) The etiology of pain in Sever disease is believed to be repetitive trauma to the weaker structure of the apophysis, induced by the pull of the tendo calcaneus (Achilles tendon) on its insertion. This results in a clinical picture of heel pain in a growing active child, which worsens with activity. Sever disease is a self-limited condition, accordingly, no known complication exists from failure to make the correct diagnosis. Causes Overuse and stress on the heel bone through participation in sports is a major cause of calcaneal apophysitis. The heel?s growth plate is sensitive to repeated running and pounding on hard surfaces, resulting in muscle strain and inflamed tissue. For this reason, children and adolescents involved in soccer, track, or basketball are especially vulnerable. Other potential causes of calcaneal apophysitis include obesity, a tight Achilles tendon, and biomechanical problems such as flatfoot or a high-arched foot. Symptoms Sever's Disease is most commonly seen in physically active girls and boys from ages 10 to 15 years old. These are the years when the growth plate is still ""open,"" and has not fused into mature bone. Also, these are the years when the growth plate is most vulnerable to overuse injuries, which are usually caused by sports activities. The most common symptoms of this disease include. Heel pain in one or both heels. Usually seen in physically active children, especially at the beginning of a new sports season. The pain is usually experienced at the back of the heel, and includes the following areas. The back of the heel (that area which rubs against the back of the shoe). The sides of the heel. Actually, this is one of the diagnostic tests for Sever's Disease, squeezing the rear portion of the heel from both sides at the same time will produce pain. It is known as the Squeeze Test. Diagnosis It is not difficult for a doctor to diagnose Sever's disease in a youngster or teenager. A personal history and a physical examination are usually all it takes to determine the cause of heel pain. Non Surgical Treatment Sever disease is heel pain in children. This pain is caused by inflammation of the heel growth plate. The growth plate is the area where the bone grows. It is located on the lower back part of the heel. Prevention Sever's disease may be prevented by maintaining good joint and muscle flexibility in the years leading up to, and during, their growth spurts (eg girls 8 to 10, boys 10 to 12). Foot arch problems such as flat feet should be addressed after the age of five if they don't appear to be self-correcting. If you are concerned, please ask your health practitioner. The most important factor is the amount of weight-bearing exercise your child is currently performing.
Overview
 The Achilles tendon is the extension from the two large muscles in the calf region, the gastrocnemius and the soleus. These two muscles combine to form the Achilles tendon. The tendon forms in the lower one third of the leg and extends to the back of the heel bone (calcaneus). When the muscles of the calf contract this produces tension on the Achilles tendon pulling on the back of heel causing the heel to rise and the foot to point downward. It is during this motion that high-tension force is transmitted through the Achilles tendon during pushing and jumping activity. This high tension force can cause the Achilles tendon to tear or rupture. This happens in 3 common locations. The most common location for a tendon tear is within the tendon substance just above the heel. The second and third most common locations are where the Achilles tendon attaches into the heel bone and higher in the leg, where the tendon begins. The Achilles tendon is the extension from the two large muscles in the calf region, the gastrocnemius and the soleus. These two muscles combine to form the Achilles tendon. The tendon forms in the lower one third of the leg and extends to the back of the heel bone (calcaneus). When the muscles of the calf contract this produces tension on the Achilles tendon pulling on the back of heel causing the heel to rise and the foot to point downward. It is during this motion that high-tension force is transmitted through the Achilles tendon during pushing and jumping activity. This high tension force can cause the Achilles tendon to tear or rupture. This happens in 3 common locations. The most common location for a tendon tear is within the tendon substance just above the heel. The second and third most common locations are where the Achilles tendon attaches into the heel bone and higher in the leg, where the tendon begins.Causes Repeated stress from a variety of causes is often the cause of Achilles tendon injury. The stress may occur from any of the following. Excessive activity or overuse. Flat feet. Poorly fitting or inadequate shoes. Inadequate warm-up or proper conditioning. Jogging or running on hard surfaces. Older recreational athlete. Previous Achilles tendon injury (tendonitis/rupture). Repeated steroid injections. Sudden changes in intensity of exercise. Use of fluoroquinolone antibiotics (especially in children). Trauma to the ankle. Tense calf muscles prior to exercise. Weak calf muscles. Symptoms Symptoms usually come on gradually. Depending on the severity of the injury, they can include Achilles pain, which increases with specific activity, with local tenderness to touch. A sensation that the tendon is grating or cracking when moved. Swelling, heat or redness around the area. The affected tendon area may appear thicker in comparison to the unaffected side. There may be weakness when trying to push up on to the toes. The tendon can feel very stiff first thing in the morning (care should be taken when getting out of bed and when making the first few steps around the house). A distinct gap in the line of the tendon (partial tear). Diagnosis Laboratory studies usually are not necessary in evaluating and diagnosing an Achilles tendon rupture or injury, although evaluation may help to rule out some of the other possibilities in the differential diagnosis. Plain radiography. Radiographs are more useful for ruling out other injuries than for ruling in Achilles tendon ruptures. Ultrasonography of the leg and thigh can help to evaluate the possibility of deep venous thrombosis and also can be used to rule out a Baker cyst, in experienced hands, ultrasonography can identify a ruptured Achilles tendon or the signs of tendinosis. Magnetic resonance imaging (MRI). MRI can facilitate definitive diagnosis of a disrupted tendon and can be used to distinguish between paratenonitis, tendinosis, and bursitis. Non Surgical Treatment Once a diagnosis of Achilles tendon rupture has been confirmed, a referral to an orthopaedic specialist for treatment will be recommended. Treatment for an Achilles tendon rupture aims to facilitate the torn ends of the tendon healing back together again. Treatment may be non-surgical (conservative) or surgical. Factors such as the site and extent of the rupture, the time since the rupture occurred and the preferences of the specialist and patient will be considered when deciding which treatment will be undertaken. Some cases of rupture that have not responded well to non-surgical treatment may require surgery at a later stage. The doctor will immobilise the ankle in a cast or a special hinged splint (known as a ?moon boot?) with the foot in a toes-pointed position. The cast or splint will stay in place for 6 - 8 weeks. The cast will be checked and may be changed during this time.  Surgical Treatment The best treatment for a ruptured Achilles tendon in an active individual is typically surgery. While an Achilles rupture can sometimes be treated with a cast, splint, brace, or other device that will keep your lower leg from moving, surgery provides less chance that the tendon will rupture again and offers more strength and a shorter recovery period. Surgery may be delayed for a period of a week after the rupture, to let the swelling go down. There are two types of surgery to repair a ruptured Achilles tendon and both involve the surgeon sewing the tendon back together through the incision. Open surgery, the surgeon makes a single large incision in the back of the leg. Percutaneous surgery, the surgeon makes a number of small incisions rather than one large incision. Depending on the condition of the torn tissue, the repair may be reinforced with other tendons. Prevention To reduce your chance of developing Achilles tendon problems, follow the following tips. Stretch and strengthen calf muscles. Stretch your calf to the point at which you feel a noticeable pull but not pain. Don't bounce during a stretch. Calf-strengthening exercises can also help the muscle and tendon absorb more force and prevent injury. Vary your exercises. Alternate high-impact sports, such as running, with low-impact sports, such as walking, biking or swimming. Avoid activities that place excessive stress on your Achilles tendons, such as hill running and jumping activities. Choose running surfaces carefully. Avoid or limit running on hard or slippery surfaces. Dress properly for cold-weather training and wear well-fitting athletic shoes with proper cushioning in the heels. Increase training intensity slowly. Achilles tendon injuries commonly occur after abruptly increasing training intensity. Increase the distance, duration and frequency of your training by no more than 10 percent each week.
Overview
Adult Acquired Flatfoot (Posterior Tibial Tendon Dysfunction) is a painful, progressive deformity in adults. It results from a gradual stretch (attenuation) of the tibialis posterior tendon and the ligaments that support your foot?s arch. This stretching causes the tendon to lose strength and function. Many people have flat feet and do not experience pain. However, pain occurs with Adult Acquired Flatfoot because the tendons and ligaments have been torn. Once the vital ligaments and posterior tibial tendon are lost, there is no longer anything holding the arch of the foot in place.  Causes Women are affected by Adult Acquired Flatfoot four times more frequently than men. Adult Flatfoot generally occurs in middle to older age people. Most people who acquire the condition already have flat feet. One arch begins to flatten more, then pain and swelling develop on the inside of the ankle. This condition generally affects only one foot. It is unclear why women are affected more often than men. But factors that may increase your risk of Adult Flatfoot include diabetes, hypertension, and obesity. Symptoms Some symptoms of adult acquired flat foot are pain along the inside of the foot and ankle, pain that increases with activity, and difficulty walking for long periods of time. You may experience difficulty standing, pain on the outside of the ankle, and bony bumps on the top of the foot and inside the foot. You may also have numbness and tingling of the feet and toes (may result from large bone spurs putting pressure on nerves), swelling, a large bump on the sole of the foot and/or an ulcer (in diabetic patients). Diabetic patients should wear a properly fitting diabetic shoe wear to prevent these complications from happening. Diagnosis It is of great importance to have a full evaluation, by a foot and ankle specialist with expertise in addressing complex flatfoot deformities. No two flat feet are alike; therefore, "Universal" treatment plans do not exist for the Adult Flatfoot. It is important to have a custom treatment plan that is tailored to your specific foot. That starts by first understanding all the intricacies of your foot, through an extensive evaluation. X-rays of the foot and ankle are standard, and MRI may be used to better assess the quality of the PT Tendon. Non surgical Treatment Conservative treatment is indicated for nearly all patients initially before surgical management is considered. The key factors in determining appropriate treatment are whether acute inflammation and whether the foot deformity is flexible or fixed. However, the ultimate treatment is often determined by the patients, most of whom are women aged 40 or older. Compliance can be a problem, especially in stages I and II. It helps to emphasise to the patients that tibialis posterior dysfunction is a progressive and chronic condition and that several fittings and a trial of several different orthoses or treatments are often needed before a tolerable treatment is found. 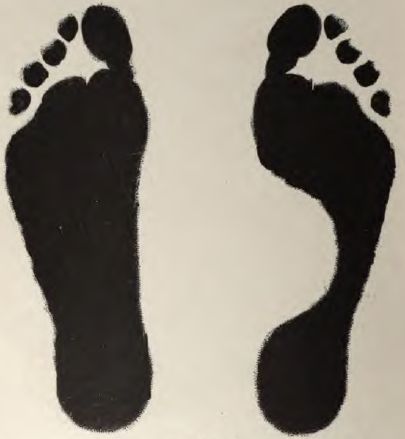 Surgical Treatment For patients with a more severe deformity, or significant symptoms that do not respond to conservative treatment, surgery may be necessary. There are several procedures available depending on the nature of your condition. Ligament and muscle lengthening, removal of inflamed tendon lining, transferring of a nearby tendon to re-establish an arch, and bone realignment and fusion are examples of surgical options to help with a painful flatfoot condition. Surgery can be avoided when symptoms are addressed early. If you are feeling ankle pain or notice any warmth, redness or swelling in your foot, contact us immediately. We can create a tailored treatment plan to resolve your symptoms and prevent future problems. |
